
Disclaimer: This information is intended as general advice only and does not replace individual medical guidance. Consult your medical professional to determine the best approach for your specific needs.
Research consistently shows that many people — particularly women — with hypermobility face significant delays in receiving a diagnosis of hEDS or Hypermobility Spectrum Disorder (HSD). Earlier studies reported diagnostic delays of 10–15 years (Blajwajs et al., 2023; Halverson et al., 2023; Trudigan & Flood, 2024).
More recent evidence suggests these delays are considerably longer. Daylor et al. (2025) — in the largest international survey of hEDS and HSD to date, with nearly 4,000 validated participants — reported mean diagnostic delays of 22.1 years for hEDS and 17.5 years for HSD.
What the research doesn’t tell us is whether a formal medical diagnosis is the right goal for everyone who is hypermobile. For many people, recognition of their condition and a clear management plan may matter far more than a diagnostic label. This article explores both sides of that question: do you actually need an official diagnosis?
New to hypermobility? Start with our blog – “What is Hypermobility?”
Can An Allied Health Professional Officially Diagnose Me with Hypermobile Ehlers Danlos Syndrome or Hypermobility Spectrum Disorder?
Experienced therapists who are familiar with hypermobility classification may be able to screen your symptoms, then determine if they meet the clinical criteria for hEDS and can give you a “provisional” or “clinical” diagnosis.
However, they cannot formally diagnose hEDS (or HSD), as international diagnostic guidelines require a medical doctor to rule out other conditions before confirming a diagnosis.
Your therapist and GP can screen for any red flags (symptoms suggestive of more serious conditions) and advise you/your team if further medical assessment is necessary.
Hypermobility is very common, and in mild or moderate cases where you are participating well in work and recreational activities, a provisional diagnosis is sufficient for effective management, as there is no curative medical treatment for hEDS or HSD, and the management approach for both conditions is largely the same.
Is An Official Medical Diagnosis Necessary?
There are pros and cons to obtaining a formal medical diagnosis. Many people with mild or moderate symptoms manage well with a supportive GP who can coordinate care and refer to other team members as needed.
Not everyone with hypermobile joints requires a formal diagnosis. If you are not symptomatic and are living comfortably, no medical diagnosis is necessary for appropriate management.
However, if your hypermobility is accompanied by pain, fatigue, frequent injuries, or other systemic symptoms, it’s advisable to seek guidance from a healthcare professional familiar with connective tissue disorders. Specialists who may assist include rheumatologists, geneticists, physiotherapists or exercise physiologists experienced in hypermobility – and women’s health or pelvic floor physiotherapists where relevant.
Receiving a diagnosis can help validate your symptoms, guide management strategies, and improve access to multidisciplinary care or allied health support. However, it’s important to consider that a formal diagnosis – especially a genetic one – may carry implications for life, income protection, and travel insurance or family planning.
Ultimately, the decision to pursue a diagnosis is a personal decision that can be discussed with your allied health team, your GP, and your family. A diagnosis should always be considered as part of the plan where it will lead to supporting your treatment, management, and overall quality of life.
Understanding the Positives and Negatives of Diagnosis
There are both benefits and drawbacks to pursuing a formal diagnosis. Understanding these can help you make an informed decision with your healthcare team:
Potential Benefits
- Validation of symptoms: You may feel heard, seen, and legitimised in your struggles. A diagnosis can end years of confusion or dismissal (Bennett et al., 2021).
- Access to support: May be required for applications for NDIS, Disability Support Pension, school accommodations, or other governmental services (Note: Unfortunately, a diagnosis does not guarantee access to these schemes.)
- Improved care coordination: Enhances communication between GPs, physiotherapists, specialists, and other allied health professionals.
- Clearer management plan: Can clarify treatment goals and help identify systemic comorbidities (e.g., POTS, MCAS).
- Empowerment through knowledge: Some people feel more in control when they understand their condition and prognosis.
Potential Drawbacks
- Risk of over-medicalisation: In cases with mild symptoms or general hypermobility, medical labelling can lead to unnecessary worry or over-identification with the diagnosis.
- Insurance implications: Diagnoses can affect life, income protection, and travel insurance, particularly a diagnosis of hEDS (due to its genetic inheritance pattern).
- No specific biomarker: hEDS is diagnosed clinically; the lack of a definitive test means diagnosis can be subjective and may vary between clinicians.
- Limited management changes: Many people with mild-moderate symptoms can be effectively managed by experienced clinicians without a formal diagnosis.
- Diagnosis without action: Receiving a diagnosis without access to appropriate multidisciplinary care can leave you frustrated or without adequate support.
- Limited professional knowledge: Unfortunately, even with a diagnosis, some health professionals may have limited understanding of hypermobility, which can lead to dismissive attitudes or inadequate care (Halverson et al., 2023).
The Diagnosis Process
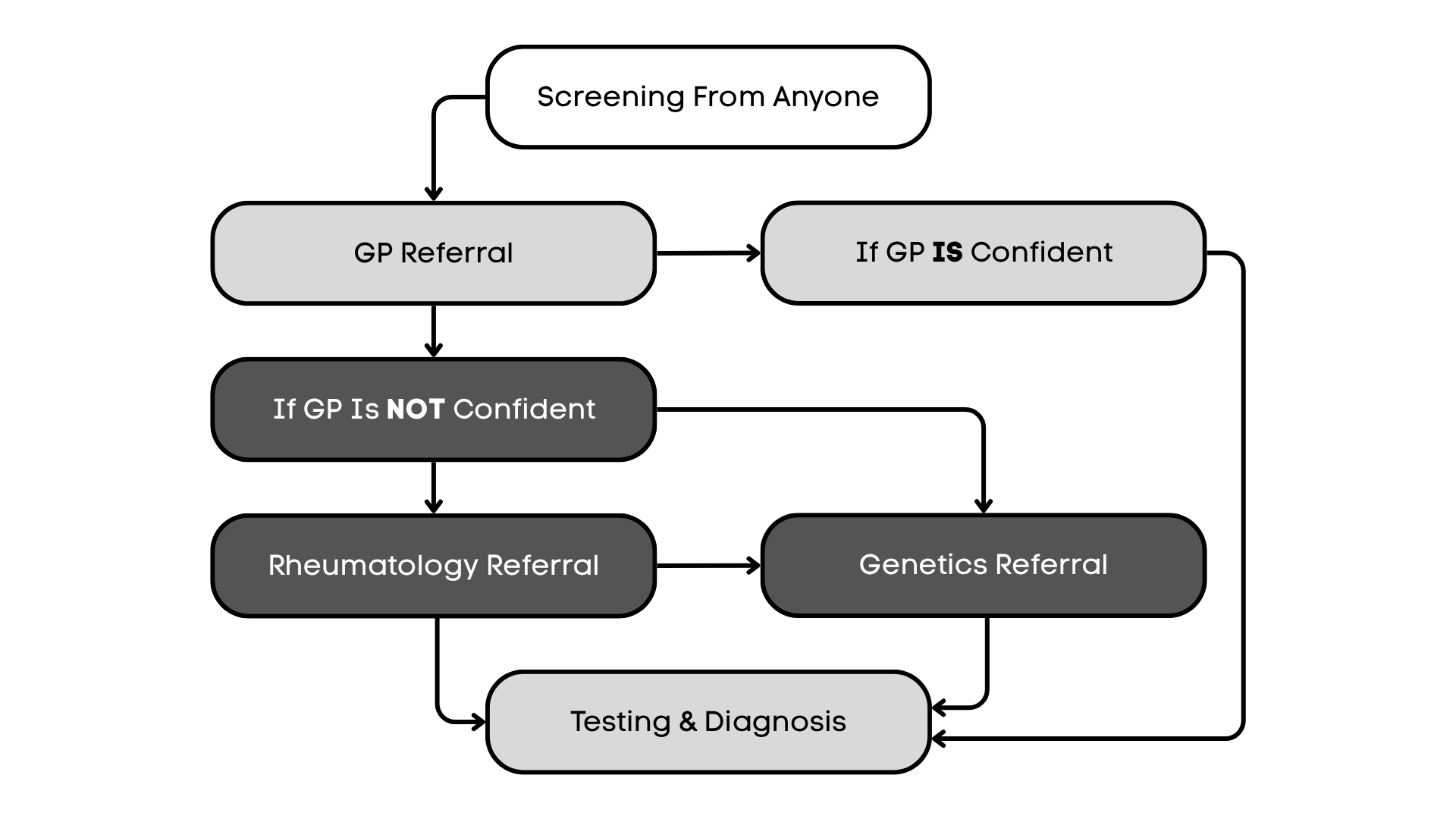
Getting a diagnosis for hEDS or HSD typically follows a pathway that begins with screening and assessment by healthcare professionals who understand hypermobility. The journey varies depending on your presentation, symptoms, and whether concerning features, sometimes called red flags, are identified during your assessment.
In many cases, your primary care doctor or General Practitioner (GP) who is confident in their assessment and finds no red flags may provide a formal diagnosis. This is often sufficient for accessing appropriate management and care.
Your GP will assist if further medical investigation is required. They may order blood tests, and in some cases, a cardiac ECHO (heart ultrasound) to screen for heart issues. They can also help set up a pain management plan for you and make referrals to appropriate health professionals.
If your GP would like the support of a specialist doctor for diagnostic clarity, you may be referred to a rheumatologist or clinical geneticist for specialist assessment.
The flowchart below illustrates the typical diagnostic pathway from initial screening through to diagnosis.
Genetic Testing and Rare Types of EDS
Is Genetic Testing Needed to Confirm hEDS?
Genetic testing is not required for diagnosing hEDS, as no specific genetic marker has been identified. International experts only recommend genetic testing when there is clear evidence of a different hereditary condition that requires elimination, in which case your doctor may refer you for testing to exclude alternative diagnoses.
Could I Have a Rare or Dangerous Type of Connective Tissue Disorder?
It is understandable to be concerned about the possibility of having a rarer and potentially more serious form of Ehlers-Danlos Syndrome (EDS) or another connective tissue disorder. Research consistently demonstrates that hEDS and HSD are more common than previously recognised (Demmler et al., 2019), while other forms of EDS remain extremely rare.
Conditions such as vascular EDS, classical EDS, Loeys-Dietz syndrome, Marfan syndrome, or osteogenesis imperfecta usually present with distinct signs and symptoms that hypermobility-aware professionals are trained to look for.
These may include the following:
Cardiovascular and Circulatory Concerns
• Artery aneurysm or dissection
• Aortic root dilation or significant valve abnormalities
• Family history of aortic dissection, aneurysm, brain bleeds, or sudden death under age 50
• A diagnosed connective tissue disorder (e.g., Marfan syndrome or Loeys-Dietz syndrome) in your family
Other Concerning Features
• Dislocation of the lens (ectopia lentis) or other eye issues (e.g., corneal thinning)
• History of pneumothorax (collapsed lung) without obvious trauma
• Rectal, uterine, or other organ rupture
• Recurrent fractures from minimal trauma, or bone fragility
• Unexplained early deaths (under age 50) in extended family (e.g., uncles or grandparents)
Why Isn’t Genetic Testing Done for Everyone?
Access to genetic testing for hypermobility is limited. The reality is there are simply not enough geneticists interested in hypermobility to do genetic screening for every individual. Government genetics services will not accept referrals for hypermobile clients, and some private services have multi-year waiting lists or only accept referrals from other medical specialists. This is a worldwide problem.
Recently, preliminary findings from the HEDGE study (1000 hEDS participants with genetic screening) have been presented (The Ehlers-Danlos Society, 2024). Of all those with a clinical hEDS diagnosis, only 7 of the 1000 (0.7%) showed genetic signs of another type of EDS or connective tissue disorder (The Ehlers-Danlos Society, 2024). This research reinforces that the vast majority of people with hypermobility symptoms do have hEDS or HSD, and that alternative rare conditions are extremely uncommon.
What About Direct-to-Consumer Genetic Testing?
It can also be tempting to access whole genome screening without the assistance of a geneticist. Unfortunately, these tests often identify many genetic variations, but the significance of these genetic variations in relation to a person’s symptoms is often not clear without appropriate genetic counselling or professional interpretation. Many experts feel that these tests are not useful for hypermobility screening and discourage their use by the general public for self-diagnosis.
Important Note: Diagnostic Criteria May Change
The diagnostic criteria for hEDS will be updated on December 1st, 2026. These changes may include additional areas of assessment beyond the current Beighton score, such as shoulder, toe, and ankle mobility. This means that some individuals who currently meet (or don’t meet) the criteria may find their classification changes when new guidelines are released.
The Most Important Part: Effective Management
Remember: obtaining a diagnosis is only the first step in your journey with hypermobility. What truly matters is effective symptom management and improving your quality of life.
Whether you have a formal diagnosis from a specialist, a provisional diagnosis from an experienced allied health professional, or are still in the process of being assessed, you can and should receive appropriate care and support. Effective management includes:
- Building a supportive relationship with your GP and healthcare team
- Working with physiotherapists or exercise physiologists experienced in hypermobility
- Developing an appropriate exercise and strengthening program
- Managing pain effectively with your medical team
- Addressing co-existing conditions (such as POTS, chronic pain, and fatigue)
- Learning pacing strategies and activity modification
- Accessing psychological support when needed
Trusted healthcare professionals who understand hypermobility can provide excellent care and support regardless of whether you have a formal diagnosis. Your symptoms, function, and quality of life are what matter most – not a label on paper.

Are You a Clinician? Learn More About Hypermobility
Led by Sharon Hennessey, the Hypermobility Project offers practical, evidence-based clinical education to help health professionals confidently recognise, manage, and treat people with hypermobility, EDS, and HSD.
Join the newsletter to be the first to know when courses launch and to download your free Red Flags Checklist — a practical reference for spotting serious pathology and knowing when to refer on.
References
- Halverson, C. M. E., Cao, S., Perkins, S. M., & Francomano, C. A. (2023). Comorbidity, misdiagnoses, and the diagnostic odyssey in patients with hypermobile Ehlers-Danlos syndrome. Genetics in Medicine Open, 1(1), 100812. https://doi.org/10.1016/j.gimo.2023.100812
- The Ehlers-Danlos Society. (n.d.). The HEDGE study. Retrieved [date], from https://www.ehlers-danlos.com/the-hedge-study/
- Bennett, S. E., Walsh, N., Moss, T., & Palmer, S. (2021). Understanding the psychosocial impact of joint hypermobility syndrome and Ehlers-Danlos syndrome hypermobility type: A qualitative interview study. Disability and Rehabilitation, 43(6), 795-804. https://doi.org/10.1080/09638288.2019.1641848
- Daylor, V., Griggs, M., Weintraub, A., Byrd, R., Petrucci, T., Huff, M., Byerly, K., Fenner, R., Severance, S., Griggs, C., Sharma, A., Atwal, P., Kautz, S. A., Shapiro, S., Youkhana, K., Lavallee, M., Wilkerson, A., Nichols, M., Snyder, A., … Norris, R. A. (2025). Defining the chronic complexities of hEDS and HSD: A global survey of diagnostic challenges, life-long comorbidities, and unmet needs. Journal of Clinical Medicine, 14(16), 5636. https://doi.org/10.3390/jcm14165636
- Blajwajs, L., Williams, J., Timmons, W., & Sproule, J. (2023). Hypermobility prevalence, measurements, and outcomes in childhood, adolescence, and emerging adulthood: A systematic review. Rheumatology International, 43(8), 1423–1444. https://doi.org/10.1007/s00296-023-05338-x
- Demmler, J. C., Atkinson, M. D., Reinhold, E. J., Choy, E., Lyons, R. A., & Brophy, S. T. (2019). Diagnosed prevalence of Ehlers-Danlos syndrome and hypermobility spectrum disorder in Wales, UK: A national electronic cohort study and case-control comparison. BMJ Open, 9(11), e031365. https://doi.org/10.1136/bmjopen-2019-031365
- Halverson, C. M., Penwell, H. L., & Francomano, C. A. (2023). Clinician-associated traumatization from difficult medical encounters: Results from a qualitative interview study on the Ehlers-Danlos syndromes. SSM – Qualitative Research in Health, 3, 100237. https://doi.org/10.1016/j.ssmqr.2023.100237
- Trudigan, R., & Flood, T. (2024). An exploration of the journey to diagnosis of Ehlers-Danlos syndrome (EDS) for women living in Australia. PLOS ONE, 19(7), e0307574. https://doi.org/10.1371/journal.pone.0307574
Want some support figuring things out?
Check out the services we offer, learn how we can help, or get in touch to book a session with our therapists.
Learn More
You can find more information curated by Not Just Bendy at:
Diagnosis
Comorbidities
- Mast Cell Activation Disorders
- Postural Orthostatic Tachycardia Syndrome (POTS)
- Exercise Tips for Postural Orthostatic Tachycardia Syndrome (POTS)
Surgery Implications
Musculoskeletal
Women’s Health
Technology
Management
Resources & Links